Oof. This comic from SMBC. https://www.smbc-comics.com/comic/funding
Oof. This comic from SMBC. https://www.smbc-comics.com/comic/funding
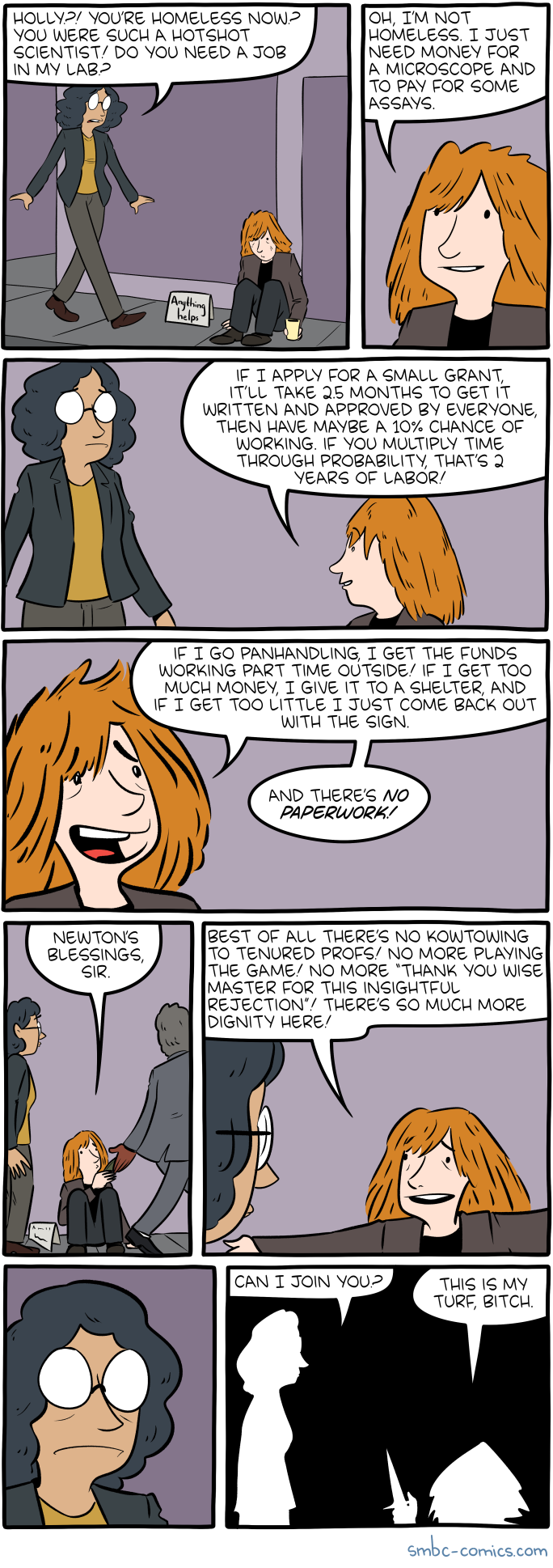
Lol. I suggested doing a clinical trial to examine whether shortening preoperative fasting times had any clinically significant costs/ benefits and was told, “Nah that would take too much time. Plus there’s this one single center study using retrospective data that shows that it affects this one surrogate endpoint in a way that has unclear clinical significance. And anyway they’ve been doing it this way in Europe for years.” And he’s right. If he pushes the protocol change through, he scores points in the department because he “did something productive for the department” whereas a trial might not even work, and produce just a few paper – maybe. And would be a ton more work. I see his point, actually. Remind me again why I am doing this?

Leave a comment